
|
|

|
A Table of Comparisons
by Lawrence Martin, MD
|
TOPIC |
ResMed ASV |
Respironics AutoSV |
Comment |
History |
For years there was just CPAP and BiPAP to treat sleep apnea patients. In 2001 a paper appeared about a novel treatment for one form of central sleep apnea: Teschler H, et al. Adaptive pressure support servo-ventilation: a novel treatment for Cheyne-Stokes respiration in heart failure. Am J Respir Crit Care Med 2001;164:614-9. The study used ResMed Corporation's new ASV machine to deliver variable pressures to patients with Cheyne-Stokes respiration -- the waxing and waning breathing often seen during sleep in heart failure patients. Soon the machine was used for treating all types of central sleep apnea as well as complex sleep apnea, a condition not recognized until after the machine was already in use. |
"ASV" as a label and a particular methodology to adjust pressures was patented by ResMed. A few years later, another large equipment manufacturer, Philips Respironics, came out with their own ASV-type machine; they call it "autoSV." Auto SV is also an adaptive servo ventilator device that uses a different algorithm to adjust bilevel pressures. A newer model is called Auto-SV Advanced (discussed below). |
ASV is but a way station on the road to newer and smarter machines. Expense (about $6000 per machine) limits their wider use, but no doubt these machines will become cheaper and at some point replace our basic CPAP/BiPAP units. |
Methodology |
The basic difference between the two devices is the way the patient's breathing is tracked so that IPAP and/or EPAP can be adjusted. Per ResMed's fact sheet, the algorithm for ResMed's VPAP Adapt SV (as their machine is called):
"uses three factors to achieve synchronization between
pressure support and the patient's breathing.
In other words, the algorithm is proprietary and unique to ResMed. To highlight this point, below is a quote about the ResMed algorithm from Brown LK. Whither adaptive servo-ventilation? Current Opinion in Pulmonary Medicine 2010;16:527-29: "The [ResMed] VPAP Adapt SV relies on a complicated estimate of recent average ventilation using mask pressure and total airflow to obtain target minute ventilation and determines respiratory phase using an estimate of intantateous respiratory airflow (and may also utilize 'fuzzy' catergories of resipratory phase). Furthermore, a host of internal constants and parameters govern the microprocessor's decisions with respect to pressure changes and cycling times, none of which are user-adjustable or explicitly stated." |
The
Philips Respironics FAQ states that the device tracks flow. "The flow signal is analyzed and
a target flow is calculated. If the patient reaches the flow target,
the device does not offer any additional pressure support. If the patient does not reach the
flow target the device will dynamically change pressure support breath to breath." Omitted
from this FAQ is that the device tracks peak flow over a 4-minute cycle, as shown below.
|
Despite the fact that the proprietary algorithms are rather opaque, both machines seem to work well in their stated objectives of treating central sleep apnea and complex sleep apnea. As such, they compete in the market for treatment of these conditions. And while each company claims its methodology is superior to the other, there is no head-to-head study. From the standpoint of the sleep medicine specialist, neither machine is clearly superior or inferior. Since ResMed was first out with an ASV machine, most of the articles in the medical literature are based on ResMed's device, but there are now several publications for autoSV as well. More importantly, this is a rapidly evolving field, and new machines will likely appear soon, from these two companies as well as other competitors. |
Pressure Curves |
ASV is a form of bilevel ventilation or "BiPAP". Click here to review BiPAP The difference is that ASV varies IPAP and/or EPAP to adjust ventilation as needed by the patient. With traditional BiPAP the pressures are set and don't vary. With ResMed's ASV the EPAP is fixed and the IPAP varies depending on the respiratory rate and air flow, measured continuously.Below is example of ASV delivered from ResMed's ASV machine. The figure
is from a
ResMed brochure, which explains the graph as
follows: "As breathing resumes and total ventilation exceeds the target,
Below is portion of a polysomnogram showing treatment of Cheyne-Stokes breathing with ASV. Figure is from: Banno K, Okamura K, Kryger MH: Adaptive Servo-Ventilation in patients with idiopathic Cheyne-Stokes breathing. J Clinical Sleep Medicine 2006; Vol 2, pages 181-186.
|
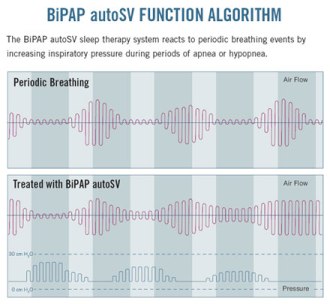
ASV is a form of bilevel ventilation or "BiPAP". Click here to review BiPAP The difference is that ASV varies IPAP and/or EPAP to adjust ventilation as needed by the patient. With traditional BiPAP the pressures are set and don't vary. With Respironics AutoSV, the IPAP and/or EPAP vary depending on a rolling average of the patient's peak air flow (see Methodology, above).Respironics currently has two machines: AutoSV and Advanced AutoSV. With regular AutoSV the EPAP is fixed and the IPAP varies. With Advanced AutoSV both EPAP and IPAP can vary. Below is the pressure curve from Repironics regular AutoSV machine, taken from a Respironics bronchure.
|
This is a rapidly evolving technology and new machines will likely come on the market soon. At this writing there is no head-to-head comparison of machines, and neither methodology has been proved superior. |
Principal Indications |
|
|
If complex sleep apnea ("CompSA") is a result of CPAP, BiPAP may be tried, though
it is not usually successful. When CompSA doesn't respond to BiPAP, or is a result
of BiPAP in the first place, there are two choices:
|
Clinical Studies |
The first clinical article on ASV appeared in 2001:
|
For studies with Respironics' AutoSV, see:Randerath WJ, et al. Adaptive servo-ventilation in patients with coexisting sleep apnoea/ hypopnoea and Cheyne-Stokes respiration. Sleep Med 2008 Dec;9:823-30 |
Again, there are no head-to-head studies. Related articles of interest include:Eckert DJ, at al. Central sleep apnea: pathophysiology and treatment. Chest. 2007;131:595-607 Gay PC.
Complex sleep apnea: it really is a disease. J Clin Sleep Medicine 2008 Oct 15;4:403-05.
Kuzniar TJ, Morgenthaler TI.
Treatment of complex sleep apnea syndrome. Curr Treat Options Neurol 2008;Sept 10;336-41.
Brown LK.
Whither adaptive servo-ventilation? Current Opinion in Pulmonary Medicine
2010;16:527-29.
|
What kind of mask is used to deliver ASV? |
ResMed recommends their full face mask. Shown below is the ResMed Quattro
Pro full face mask.
|
Respironics states any mask used for CPAP should work with their autoSV machine.
Below is the Respironics Comfort Gel full face mask.
|
Mask type and size is best determined in the sleep lab, when a patient is being titrated on an ASV machine. |
Prescription Examples |
ResMed VPAP Adapt SV:
|
Respironics currently has TWO devices on the market, the regular AutoSV and the AutoSV Advanced. Respironics recommends that physcians now prescribe ONLY the AutoSV Advanced, so it seems likely that the regular machine will be phased out soon. Below are prescription examples for both.
Regular AutoSV
Prescribing AutoSV Advanced
|
The technology is evolving and this section should change as new machines (and methods of delivering ASV) come on the market. |
Medicare Coverage Guidelines(To some extent these guidelines also influence most commercial insurance coverage) |
The following information is from the CMS web site on Respiratory Assist Devices
for Central sleep apnea, defined as:
for Complex sleep apnea
| Same criteria as for ResMed |
NOTE: CMS defines an hypopnea as "an abnormal respiratory event lasting at least 10 seconds associated with at least a 30% reduction in thoracoabdominal movement or airflow as compared to baseline, and with at least a 4% decrease in oxygen saturaiton." This definition makes the CMS criteria for central sleep apnea and CompSA confusing, because hypopneas are not traditionally scored as obstructive or central, but simply 'hypopneas'. Thus by CMS criteria a patient could have persistently high AHI from obstructive hypopneas after a CPAP/BiPAP titration, yet qualify for an ASV machine. One doubts that was the intent of the stated criteria. Perhaps even more amazing is that all the DME companies quote the CMS guidelines, and never stop to explain the role of hypopneas in defining central sleep apnea. For example, see the Respironics brochure that details how to prescribe their auto SV unit. |
Web sites for more information |
RESMED WEB SITES |
RESPIRONICS WEB SITES |
Please refer to 'Clinical Studies' for discussion of ASV in general.
|
Costs |
ResMed's VPAP Adapt SV is not sold new on the internet, but is probably the same price as Respironics AutoSV machine, which is $5800 at cpap.com. In addition there is the cost of the mask, and also the sleep studies needed before any machine can be prescribed. |
At cpap.com the Remstar Auto SV is $5800 for the machine alone. In addition there is the cost of the mask, and also the sleep studies needed before any machine can be prescribed. |
There are many web sites for purchasing CPAP machines, including: cpap.com, CPAP-Supply and The CPAP Shop.In clinical practice patients usually get their machine from a DME (durable medical equipment) company, following a physician's prescription. The DME cost of positive pressure devices is generally higher than the cost when purchased on the internet, because the DME companies provide service to the machine and training to the patient. Even so, DME companies will generally accept whatever the insurer pays, as long as it covers their cost. The insurer will sometimes rent the machine from the DME company, sometimes buy it outright, and there may or may not be a deductible to the patient. Thus there is no simple answer. |
|
Return to Table: ResMed vs. Respironics
Return to Home Page: CPAP, BiPAP, ASV
Return to Lakeside Press home page
Forward any comments to:
larry.martin@roadrunner.com
 A peak flow target is established around the 4-minute average and the machine changes
the air delivery as needed, to deliver 95% of the target, as shown below.
A peak flow target is established around the 4-minute average and the machine changes
the air delivery as needed, to deliver 95% of the target, as shown below.





{kind=link}
{kind=link}
{kind=link}