|
|
|
PaO2, SaO2 and Oxygen ContentThe following section is adapted from Chapter 5 of All You Really Need to Know to Interpret Arterial Blood Gases.
In the field of blood gas interpretation, confusion
about PaO2, SaO2 and oxygen content is second only to confusion
about mixed acid-base disturbances.
Arterial PO2 (little 'a')gives us valuable
information about adequacy of gas exchange within the lungs, when (and only when) it is
subtracted from the calculated alveolar PO2 (big A). We use the
Alveolar Gas Equation to calculate PAO2.
The difference between measured PaO2 and calculated PAO2
is called the Alveolar-arterial PO2 difference or 'A-a Gradient' for short.
The A-a gradient answers the important question: Are the lungs
transferring oxygen properly from the atmosphere to the pulmonary circulation? If the A-a
gradient is elevated, the answer is NO. If the A-a gradient is normal is YES. (The A-a
gradient is discussed in detail in Chapter 4).
There is a second, equally important question concerning oxygen and
gas exchange, which is the subject of this section: Of these three values, PaO2, or oxygen pressure, is the least
helpful to answer the question about oxygen adequacy in the blood.
The other two values --oxygen saturation and oxygen content --
are more useful for this purpose. I will briefly define
these three terms and then present a more detailed discussion of each, with emphasis
on their inter-relationships.
OXYGEN PRESSURE: PaO2.
Oxygen molecules dissolved in plasma (i.e., not bound to
hemoglobin) are free to impinge on the measuring oxygen electrode. This "impingement" of free
O2 molecules is reflected as the partial pressure of oxygen; if the sample being tested is arterial
blood, then it is the PaO2. Although the number of O2 molecules dissolved in plasma determines,
along with other factors, how many molecules will bind to hemoglobin, once bound the oxygen
molecules no longer exert any pressure (bound oxygen molecules are no longer free to impinge
on the measuring electrode). Since PaO2 reflects only free oxygen molecules dissolved in plasma
and not those bound to hemoglobin, PaO2 cannot tell us "how much" oxygen is in the blood; for
that you need to know how much oxygen is also bound to hemoglobin, information given by the
SaO2 and hemoglobin content. OXYGEN SATURATION: SaO2.
Binding sites for oxygen are the heme groups, the Fe++-porphyrin
portions of the hemoglobin molecule. There are four heme sites, and hence four oxygen
binding sites, per hemoglobin molecule. Heme sites occupied by oxygen molecules
are said to be "saturated" with oxygen. The percentage of all the available heme binding
sites saturated with oxygen is the hemoglobin oxygen saturation (in arterial blood, the
SaO2). Note that SaO2 alone doesn't reveal how much
oxygen is in the blood; for that we also need to know the hemoglobin content.
OXYGEN CONTENT: CaO2.
Tissues need a requisite amount of O2 molecules for metabolism.
Neither the PaO2 nor the SaO2 provide information on the number of oxygen molecules, i.e., of
how much oxygen is in the blood. (Note that neither PaO2 nor SaO2 have units that denote any
quantity.) Of the three values used for assessing blood oxygen levels, how much is provided only
by the oxygen content, CaO2 (units ml O2/dl). This is because CaO2 is the only value that
incorporates the hemoglobin content. Oxygen content can be measured directly or calculated by
the oxygen content equation (introduced in Chapter 2):
You wish it was this simple, huh? I have shown the 3 short paragraphs above to dozens of students, interns, residents; almost all will say they understand the differences, no problem. But, when given questions to test their understanding, they flub. So more instruction is needed (and, yes, a few problems along the way). Understanding the differences between PaO2, SaO2 and CaO2 is essential to proper blood gas interpretation. By the end of this and the next chapter -- if you work on all the problems -- you should be able to teach the subject! PaO2, the partial pressure of oxygen in the plasma phase of arterial blood, is registered by an electrode that senses randomly-moving, dissolved oxygen molecules. The amount of dissolved oxygen in the plasma phase -- and hence the PaO2 -- is determined by alveolar PO2 and lung architecture only, and is unrelated to anything about hemoglobin. (With one exception: when there is both anemia and a sizable right to left shunt of blood through the lungs. In this situation a sufficient amount of blood with low venous O2 content can enter the arterial circulation and lead to a reduced PaO2. However, with a normal amount of shunting, anemia and hemoglobin variables do not affect PaO2.) Oxygen molecules that pass through the thin alveolar-capillary membrane enter the plasma phase as dissolved (free) molecules; most of these molecules quickly enter the red blood cell and bind with hemoglobin (Figure 5-1). There is a dynamic equilibrium between the freely dissolved and the hemoglobin-bound oxygen molecules. However, the more dissolved molecules there are (i.e., the greater the PaO2) the more will bind to available hemoglobin; thus SaO2 always depends, to a large degree, on the concentration of dissolved oxygen molecules (i.e., on the PaO2).
Because there is a virtually unlimited supply of oxygen molecules in the atmosphere, the dissolved O2 molecules that leave the plasma to bind with hemoglobin are quickly replaced by others; once bound, oxygen no longer exerts a gas pressure. Thus hemoglobin is like an efficient sponge that soaks up oxygen so more can enter the blood. Hemoglobin continues to soak up oxygen molecules until it becomes saturated with the maximum amount it can hold - an amount that is largely determined by the PaO2. Of course this whole process is near instantaneous and dynamic; at any given moment a given O2 molecule could be bound or dissolved. However, depending on the PaO2 and other factors, a certain percentage of all O2 molecules will be dissolved and a certain percentage will be bound (Figure 5-1). In Figure 5-1, the free or dissolved oxygen molecules register a partial pressure of 95 mm Hg and the red blood cells contain a total hemoglobin content of 15 gm/dl. Each hemoglobin molecule has four Fe++heme sites for binding oxygen. If there is no interference (as from carbon monoxide, for example), the free O2 molecules bind to these sites with great avidity. The total percentage of sites actually bound with O2 is constant for a given set of conditions, and is the 'saturation of blood with oxygen'. This is called SvO2 and SaO2 in the venous and arterial circulations, respectively; in Figure 5-1, the respective values are 75% and 97%. An SaO2 of 97% simply means that of every 100 hemoglobin binding sites, 97 are occupied with an oxygen molecule and the other three are either bound to something else or are unbound.
In summary, PaO2 is determined by alveolar PO2 and the state of the alveolar-capillary interface, not by the amount of hemoglobin available to soak them up. PaO2, in turn, determines the oxygen saturation of hemoglobin (along with other factors that affect the position of the O2-dissociation curve, discussed below). The SaO2, plus the concentration of hemoglobin (15 gm/dl in this example), determine the total amount of oxygen in the blood or CaO2 (see equation for CaO2). For the variables shown in Figure 5-1, the CaO2 is 20 ml O2/dl.
From the forgoing discussion the following observations should now be apparent.
Neither the amount of hemoglobin, nor the binding characteristics of hemoglobin, should affect the amount of dissolved oxygen, and hence should not affect the PaO2). Stated another way, the number of dissolved oxygen molecules is independent of the amount of hemoglobin or what is bound to it. To repeat one more time (because it is so important), PaO2 is not a function of hemoglobin content or of its characteristics, but only of the alveolar PO2 and the lung architecture (alveolar-capillary interface). This explains why, for example, patients with severe anemia or carbon monoxide poisoning or methemoglobinemia can (and often do) have a normal PaO2. The most common physiologic disturbance of lung architecture, and hence of a reduced PaO2, is ventilation-perfusion (V-Q) imbalance. Less common causes are reduced alveolar ventilation, diffusion block, and anatomic right to left shunting of blood.
SaO2 is
determined mainly by PaO2. The relationship between the
two variables is the familiar oxygen dissociation curve (Figure 5-2A).
The dissociation curve is experimentally determined from in vitro
titration of blood with increasing partial pressures of oxygen. At low
oxygen pressures there is relatively little increase in SaO2 for a given
change in PaO2. Above a PaO2 of 20 mm Hg, the rate of change of
SaO2 increases markedly, then slows again beyond a PaO2 of 60 mm
Hg.
PaO2 is the most important (but not the only) determinant of SaO2.
Other determinants of SaO2 for a given PaO2 are conditions that shift
the position of the oxygen dissociation curve left or right, such as
temperature, pH, PaCO2 and level of 2,3-DPG in the blood. Shifts of
the O2-dissociation curve will be discussed further in the next chapter.
For now, consolidate your understanding of the difference between PaO2 and SaO2. Think of PaO2 as the driving pressure for oxygen molecules entering the red blood cell and chemically binding to hemoglobin; the higher the PaO2, the higher the SaO2. Whatever the SaO2, its value is simply the percentage of total binding sites on arterial hemoglobin that are bound with oxygen, and can never be more than 100%. Figure 5-2 (click to enlarge). 
The oxygen dissociation curve, showing PaO2 vs. SaO2 and PaO2 vs. oxygen content for two different hemoglobin values. P50 is the PaO2 at which hemoglobin is 50% saturated with oxygen; normal value is 27 mm Hg. (X represents blood gas values of a case presented in Chapter 6). The Arterial oxygen content is shown for two hemoglobin vaues, 15 gm/dl and 10 gm/dl. The relationship between SaO2 and CaO2 for any given hemoglobin content is linear (excluding the minor influence of dissolved oxygen with normal PO2 values).
The so-called "steep part" of the O2 dissociation curve is between 20 and 60 mm Hg PaO2. Compared with the flatter portions, small increases in PaO2 in this region have a much greater effect on improving SaO2 and therefore O2 content. Figure 5-2A shows the oxygen dissociation curve for PaO2 plotted against oxygen content for two hemoglobin concentrations, 15 gm% and 10 gm%. Note that the shape and position of the curve are the same irrespective of the hemoglobin content. SaO2 is unaffected by the hemoglobin content, so anemia does not lower SaO2. The more hemoglobin, the more oxygen molecules will be bound in a given volume of blood, but the percentage of available hemoglobin sites bound to oxygen (the SaO2) depends only on the PaO2 and curve-shifting factors. Thus, a patient can have a normal PaO2 and SaO2, but still have a low CaO2 (e.g., with anemia). CaO2, unlike either PaO2 or SaO2, directly reflects the total number of oxygen molecules in arterial blood, both bound and unbound to hemoglobin. In contrast to the other two variables, CaO2 depends on the hemoglobin content and is directly related to it; other determinants of CaO2 are the SaO2 (in turn dependent on PaO2 and position of the oxygen dissociation curve), and the amount of dissolved oxygen (the PaO2). Since the dissolved oxygen contributes minimally to CaO2 under physiologic conditions, CaO2 is determined almost entirely by hemoglobin content and SaO2, and is related linearly to either variable (Figure 5-2B). Normal CaO2 ranges from 16 to 22 ml O2/dl. Because PaO2 and/or SaO2 can be normal in certain conditions associated with hypoxemia, one should always make sure CaO2 is adequate when assessing oxygenation. About 98% of the normal O2 content is carried bound to hemoglobin. The CaO2 component bound to hemoglobin can be calculated by (Hb x 1.34 x SaO2) and the dissolved component by (.003 x PaO2). This equation can be used to calculate oxygen content of any blood or plasma sample.
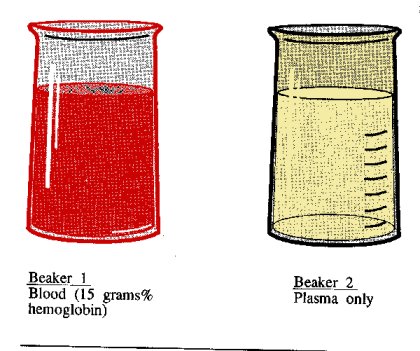
Figure 5-3 shows two beakers containing liquid open to the atmosphere. Beaker 1 contains blood with a Hb content of 15 grams%. Beaker 2 contains only plasma (no hemoglobin). Assuming a barometric pressure of 760 mm Hg (and no water vapor pressure), calculate the oxygen content in each beaker. Figure 5-3.
Beaker 1 contains blood with a hemoglobin content of 15 grams%; beaker 2 contains pure plasma, no hemoglobin. Both beakers are open to the atmosphere (dry air; barometric pressure 760 mm Hg). Beaker 1 contains hemoglobin that will combine chemically with oxygen; hence the oxygen content in beaker 1 consists of bound and unbound (dissolved) oxygen molecules. In beaker 2 there is no hemoglobin, just pure plasma; all of its oxygen content must come from dissolved oxygen. Dissolved oxygen in both beakers is determined by the PO2 to which the liquid is exposed and the solubility of oxygen in plasma. The solubility is .003 ml O2/dl plasma/mm Hg. But what is the PO2? Because there is no CO2 exchange taking place in either beaker (as there is in our lungs) and the surface of the liquid is in free contact with the atmosphere, the PO2 in solution is simply the PO2 above the solution. Given a barometric pressure of 760 mm Hg (dry air), the PO2 in both beakers is Since the PO2 is equal in both beakers, the O2 content represented by dissolved oxygen is also the same in both beakers; this content is ? a) .48 ml O2/dl b) 2.0 ml O2/dl c) 4.8 ml O2/dl To calculate content from dissolved oxygen, substitute the values for oxygen solubility and PO2: O2 content of dissolved O2 = .003 ml O2/dl/mm Hg x 160 mm Hg = .48 ml O2/dl There is no hemoglobin in beaker 2 so the entirety of its O2 content comes from dissolved oxygen and = .48 ml O2/dl. There is far more oxygen content in beaker 1 because oxygen molecules combine chemically with hemoglobin. Once combined, O2 molecules no longer exert any pressure. As O2 molecules are taken up by hemoglobin, additional molecules enter the plasma portion of the blood from the atmosphere. (Remember: Hemoglobin is like a sponge that soaks up free oxygen molecules and allows many more to enter the surrounding plasma.) Thus the difference in oxygen content between the two beakers is the amount of oxygen bound to hemoglobin. The oxygen content represented by hemoglobin-bound oxygen in beaker 1 is ? a) .48 ml O2/dl b) 15 ml O2/dl c) 19.9 ml O2/dl O2 content is calculated by the oxygen content equation, which in turn requires knowledge of SaO2, the saturation of hemoglobin with oxygen. SaO2 is determined by the PO2 to which the blood is exposed in the lungs (in this case 160 mm Hg) and the position of the oxygen dissociation curve. With a normally-positioned curve, the SaO2 at this level of PO2 is approximately 99%. Thus, Oxygen content (Hb-bound) = Hb x 1.34 x SaO2 = 15 x 1.34 x .99 = 19.9 ml O2/dl ? What is the total oxygen content of beaker 1? By what factor is this content greater than that in beaker 2? The total oxygen content of beaker 1 is of course the sum of the dissolved and bound fractions, or .48 + 19.9 = 20.38 ml O2/dl. The total oxygen content of beaker 2 (.48 ml O2/dl) is thus only about 2.4% of that contained in beaker 1. Put another way, beaker 1 contains about 42 times more oxygen than beaker 2. Clinical Problem 5-4. A healthy man is in the same room as the two beakers shown in Figure 5-3. If his PaO2 = 100 mm Hg and Hb content = 15 gms%, what percent of his oxygen content is carried in dissolved form? To summarize much of the forgoing discussion:
Clinical Problem 5-5. For each of the four conditions below, give the expected changes (increased, decreased, or normal) for PaO2, SaO2 and CaO2. Assume the subject is breathing ambient air, that each situation occurred acutely (in less than 24 hours), and that there is no other abnormal condition.
Clinical Problem 5-6. Which patient is more hypoxemic? Patient A: PaO2 85 mm Hg, SaO2 95%, Hb 7 gm% Patient B: PaO2 55 mm Hg, SaO2 85%, Hb 15 gm% Clinical Problem 5-7. Test your understanding by answering the following statements a-h as either True or False. a. If the lungs and heart are normal, then PaO2 is affected only by the alveolar PO2. b. In a person with normal heart and lungs, anemia should not lower the PaO2. c. PaO2 will go up in a patient with hemolysis of red blood cells, as dissolved oxygen is given off when the cells lyse. d. As the oxygen dissociation curve shifts to the right, PaO2 rises since less oxygen is bound to hemoglobin. e. An anemic patient who receives a blood transfusion should experience a rise in both SaO2 and CaO2. f. The PaO2 in a cup of water is zero since there is no blood perfusing the water. g. The SaO2 in a cup of water is zero since there is no hemoglobin present. h. The CaO2 in a cup of water is zero since there is no hemoglobin present. Lawrence Martin, M.D. Answers to Problems Alphabetical Index to all web sites / Subject Index to all web sites |